
Puede leer aquí la versión en español de este artículo.
This article is part of the series “La Letra de Temas 2020 – Postpandemia: where to now?”
As a result of COVID-19’s peak having been reached, Temas-Catalejo asked a group of researchers to study the current status and the outlook for the rest of the year in Cuba. They were asked for a detailed diagnostic, examining not only the pandemic itself and its clinical aspects but also public health, and its socioeconomic, political, international and subjective ramifications—as well as the probable future.
In contrast to the haze of figures, received truths, declarations and reports that inundate the media, of hopes and recommendations directed to the government and which—as is common in the networks—pretend to be analysis, this series is directed towards figuring out the present and the future of the country in order to understand it better, like a road between politics and its circumstance.
As per the standard of Catalejo, La Letra de Temas 2020 is more receptive to other analyses than to other opinions.
In December of 2019, an outbreak of pneumonia of unknown origin and often fatal outcome made its appearance among people associated with a market of seafood and live animals in the city of Wuhan, China (Yang et al, 2020). Days later, health authorities in that country revealed that the epidemic outbreak that had erupted in that area was produced by a new coronavirus (named thus because of the spicules that cover its surface, in the shape of a crown) (Hui et al, 2020). The World Health Organization (WHO) named the unknown disease COVID-19 (from the English: Coronavirus Disease of 2019) (WHO, 2020a).
The virus of Wuhan, as it became known at first, is the result of the transmission and mutagenic alteration of a virus that resides in bats (Andersen et al, 2020). Only six coronaviruses had affected human beings previously. Four of these hardly cause mild symptoms, like the common cold; the other two had already caused pandemics. In 2002-03, SARS-CoV (Severe Acute Respiratory Syndrome Coronavirus) caused an epidemic that reached a fatality rate of 10%. In 2012 the MERS-CoV (Middle East Respiratory Syndrome Coronavirus) triggered an even more devastating epidemic, with a mortality index of 37% (Rabi et al, 2020).
On January 9th, 2020, Chinese researchers described and disseminated the genetic sequence of the new coronavirus (Zhou et al, 2020a). It has a 79.5% coincidence with the SARS CoV virus, because of which, by proposal of the International Taxonomy Committee, the Virus of Wuhan was renamed SARS CoV-2 (Gorbalenya et al, 2020). After recognizing the new disease and identifying its causal agent, Chinese authorities launched an intense containment campaign. However, the movement of travelers from and to the Asian nation had already spread the new coronavirus and its associated illness. The broad propagation of COVID-19 led the WHO to recognize it as a pandemic on March 11, 2020 (WHO, 2020b). Having now transformed into a major health problem with economic and social consequences, COVID-19 has reached ominous growth (westwards first, and then towards the south) to 185 countries in all continents, and has left its mark: 9,843,073 people infected and 495,760 deaths by June 28th, 2020 (WHO, 2020c).
Brief notes on the interaction between SARS CoV-2 and its human host
The cascade of pathogenic events unleashed by SARS CoV-2 begins when it penetrates a cell of the host’s respiratory system, a complex process that takes place in three steps which we shall briefly describe below.
First, the glycoprotein of one of the spicules on the surface of the virus binds up with the angiotensin-converting enzyme 2, or ACE2, which is its receptor in the cell that is being infected (see Illustration). Then, the transmembrane serine protease 2 (TMPRSS2), also present in the membrane of the host cell, bonds with ACE2 and splits into two fragments—a process by which the glycoprotein of the spicule is activated, And, finally, there is a fusion of both ligands and the penetration of the virus into the interior of the cell, in which it will begin replicating (Rabi et al, 2020).
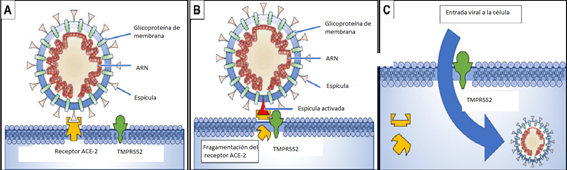
- The glycoprotein of one of the spicules on the surface of the virus binds to the ACE2 receptor on the surface of the target cell;
- The TMPRSS2 enzyme splits the ACE2 molecule and through this process the spicule’s glycoprotein is activated;
- The fragmentation of ACE2 and the activation of the spicule facilitate the penetration of the virus.
(Copied, partially modified, from Rabi, 2020).
After the initial start of the infection, the subsequent development of COVID-19 is extremely variable. It oscillates between an asymptomatic progression or mild clinical manifestation—which usually occurs in children and healthy adults—, and the development of pneumonia and serious multi-organ failures—which is more frequent in older people and patients with chronic diseases. This wide spectrum of clinical manifestations is a consequence of another one, at the immunological level: the SARS CoV-2 infection awakens innate immunological and adaptive responses which, in the most frequent and benign of the developments lead to the containment of the viral replication and to recovery, and in the most unfavorable outcome can arouse an intense inflammatory pulmonary reaction which, leading to more severe complications, can result in death (Wang et al, 2020; Cao, 2020).
COVID-19 and age
Without there being a strictly lineal relationship, most of the advisories report the risk of suffering from COVID-19 increasing with age (Shim et al, 2020). As has been indicated, in children and young adults the infection is often asymptomatic or results in mild clinical manifestations. In older person the development can be less favorable and can occasionally result in severe clinical cases.
The totality of the studies published on the topic of COVID-19 and age report the possibility of death resulting from the virus to be greater after the age of 60 (Yang et al, 2020; Rabi et al, 2020; Shim et al, 2020). In Cuba, for example, by May 5th, 2020, 79.7% of deaths caused by COVID-19 were of persons over 60. Contributing to this are other factors related to old age, in particular the presence of chronic diseases (the so-called comorbidities), which are more frequent as one passes towards a more advanced age, and the aging of immune system (Yang et al, 2020; Rabi et al, 2020; Shim et al, 2020; Márquez et al, 2020).
Regarding the comorbidities, there are four that are most often associated to COVID-19: arterial hypertension, cardiovascular diseases, diabetes mellitus, and chronic respiratory insufficiency (the order of this series depends on the population in which the study was carried out) (Yang et al, 2020). To a major or minor degree, these diseases and chronic syndromes share two characteristics which make those people who suffer from them more vulnerable to the development of severe COVID-19: the sustained presence of a pro-inflammatory state, and the relative incapacity to develop adequate immune responses to a broad variety of infectious agents (Márquez et al, 2020).
From a dynamic perspective, our immune system consists of two branches which—despite some overlaps—have different functions: the innate immune system and the adaptive one. With the aging process, both suffer changes in their cellular composition and in the quality of their functioning.
The innate immune system is the first line of defense against germs that can invade us (for example, SARS CoV2), and the inflammatory response is its primary component. Typically, when a pathogen breaks out in our tissues, it generates an acute inflammatory response which, by accumulating proteins and cells in the damaged area, removes the invader and begins the process of repair (Rabi et al, 2020). Aging is characterized by a chronic activation of the innate immune system, which results in a state of permanent inflammation that has become known as “inflamm-aging”, and which is in many ways adverse to the aging organism (Fulop et al, 2018). In other words, the innate immune response, which is favorable in young people and healthy adults, can convert itself into a potentially prejudicial mechanism in aging. The permanent activation of the inflammatory response in the elderly, which is more intense in males, has been related to the forceful pulmonary inflammation that characterizes the severe cases of COVID-19 in that age group.
The adaptive immune system is mobilized when the innate immune system is insufficient to eliminate a threat. While the innate immune system acts rapidly by the recognition of microbes through its general characteristics, the principal cells of the adaptive immune system (the B and T lymphocytes) can eliminate the invader specifically through the recognition of these microbes’ small structures, called antigens. After eliminating the foreign element, the organism conserves a large group of B and T lymphocytes, called a “memory”, which allows it to recognize and eliminate the microbe specifically and rapidly in the case of further attacks (Rabi et al, 2020).
In any phase of life, in order to assemble an effective immune response, it is necessary to have an adequate balance and cooperation between the innate and the adaptive responses. However, with the passing of the years, especially after middle age, this balance goes through a gradual decline (Goronzy & Weyand, 2017; Fulop et al, 2018). At an advanced age, the “inflamm-aging”—a consequence of the chronic activation of innate immunity—is combined with a weakening of the adaptive immune functions. This decline, which is also more pronounced in the male sex, is characterized by two constraints:
- The lack of recognition of new threats due to the reduction of the number of natural cells that could be “educated” to respond specifically to the new microbes, and
- The incapacity to develop adequate responses due to the accumulated overstimulation “for life” that has relatively “exhausted” the available immune cells (Rabi et al, 2020).
The decline in the adaptive immunity in elderly people has been related to lymphopenia (a reduced number of lymphocytes in circulating blood), fundamentally of T-cells, which characterize the severe cases of COVID-19 in people of this age (Qin, 2020).
Medicine based on sex and gender: the case of Covid-19
In the following paragraphs, with the word ‘sex’ we will be referring to the genetic and biological status of the XX or XY organisms (Yurdakök, 2020), and with the term ‘gender’ we will be referring to the roles, characteristics and opportunities which—as defined by society—are considered proper to men, women, boys, girls and people with non-binary identities (WHO, 2020).
During the last two decades, the number of publications on studies that show the influences of sex and gender on the forms of the presentation, evolution, diagnostic and treatment of multiple diseases has grown rapidly (Yurdakök, 2020; Walter & McGregor, 2020). The growing interest in these aspects forms part of a more general subject, that of precision medicine, which believes that the approach to the study of any illness can be modified based on a given segment of the population (for example, females or males). During the last few years, this line of thinking has led to what is known today as Sex and Gender Based Medicine (SGBM) (Yurdakök, 2020; Walter & McGregor, 2020).
SGBM stimulates the recognition of the influence of sex and gender in the health-illness balance and promotes the scrutiny of these variables both in research and in clinical practice. Differences of sex and gender have been observed in the evolution, diagnostic, treatment and control of clinical events of very different varieties, from cardiovascular diseases to sports injuries (Walter & McGregor, 2020). A good example in the context of the topic we are dealing with are the SARS (2003) and MERS (2012) epidemics, which had higher fatality rates in men than in women (21.9% and 13.2% resp.) (Channappanavar et al, 2017; Matsuyama et al, 2016).
The first reports on the COVID-19 epidemic in China showed a predominance of the male sex among the people infected (Gebhard et al, 2020a; Chen et al, 2020). However, after several weeks of the appearance of the first cases, the difference in the proportions of women and men among the infected individuals was not statistically significant. The initial predominance of men among infected persons was interpreted as being a consequence of there being a higher number of individuals of the male sex among the workers and assistants in the market of Wuhan.
On April 30th, 2020, 35 countries already grouped the epidemiological data of confirmed cases of the SARS CoV-2 infections by sex. Until then, 14 nations reported a higher proportion of male positives, two a similar incidence of men and women, and 19 a slightly higher quantity of females. Clearly, and as other authors reported in information published for their countries, there does not seem to be any sexual difference in regards to the absolute numbers of infection cases (Gargaglioni & Marques, 2020). Cuba does not break with this general consideration, and thus, on June 28th, 2020, of the 2,340 people infected, 1,162 (49.6%) were female and 1,178 (50.4%) male (MINSAP, 2020).
In the account of the 35 countries to which we were referring, 33 nations reported that the number of deaths by COVID-19 was much higher for men than for women. For example, until that date, the fatality rate in China was 4.7% in persons of the male sex, and 2.8% in females. That is, in this Asiatic country 68% more men than women died from COVID-19 (Gargaglioni & Marques, 2020). And Cuba does not break with this general tendency. With data from last June 28th, fatality among infected males was 4.4% and among women in the same situation, 3.0% (MINSAP, 2020).
Grouped according to sex, a very recent study analyzes the epidemiological information relating to the progress of the virus through six countries (China, Italy, Spain, France, Germany and Switzerland). Based on the 227,219 cases of people with confirmed infections of SARS CoV-2, a very important fact was observed: the fatality rate for men is consistently higher in all age ranges (Gebhard et al, 2020). This means that, independently of the fact that a similar number of men and women are infected by SARS CoV-2, proportionally more people of the male sex die at all age levels. From a more holistic perspective, this indicates that, in addition to the comorbidity and immunological senescence (which both generally gain dominance after the age of 60), factors specific to sex and gender—which we will discuss below—also increase vulnerability to COVID-19.
Factors specific to sex as related to COVID-19
In 1980, Pickering and Christie were the first to reveal the efficacy of the defensive mechanisms as associated to gender, demonstrating that female fish resisted ectoparasite attacks better than their male counterparts (Pickering & Christie, 1980). During the following decades, these differences were corroborated in other, phylogenetically more highly evolved species. In the domestic rat, for example, susceptibilities unlike the SARS CoV infection were detected. In laboratory conditions, the fatality rate in male rats infected by this virus was 90%, much higher than the 20% registered in female rats. (Channappanavar et al, 2017). From this result can be deduced from that, at least as far as coronavirus infections are concerned, rats exhibit a sexual dimorphism that is similar to lower species and to what is now being documented for humans with regard to SARS CoV2 (Walter & McGregor, 2020; Gebhard et al, 2020).
Apparently the disparity between men and women with regard to COVID-19 is part of a more general phenomenon that evolved with biparental reproduction. It is likely that a more efficient immunity system in female vertebrates (fish, rats, humans) can “confer an advantage for survival to its descendants”—a characteristic that probably evolved by the selective pressure of continuous pathogenic micro-organism attacks. Given that the males cannot “become pregnant” and “become mothers”, an “optimized immune response” did not develop in them during the evolutionary stages (Kutschera, 2020).
Women develop stronger innate and adaptive immune responses than men. This higher immunological strength has positive and negative consequences for women. In general, it makes them more resistant to infections by viruses, bacteria, fungi and parasites, and, also very interesting, gives them better responses to vaccines. However, and very much in relation to their capacity to develop stronger immune responses, women are more likely to suffer from clinical matters related to immunological hypersensitivities, especially auto-immune diseases (among them: lupus erythematosus and rheumatoid arthritis) (Klein & Flanagan, 2016; Schurz et al, 2019).
The X chromosome contains the largest number of genes of the human genome related to the manifestation and control of the immune responses (Klein & Flanagan, 2016; Jaillon et al, 2017). Women have two X chromosomes, and although a fragment of one of them is inactive, an important portion of these genes can express themselves in a dual way and give the feminine sex more robust immune responses (Klein & Flanagan, 2016; Jaillon et al, 2017). For example, the gene that codifies the molecule TLR7 (Toll-like receptor 7) escapes the X chromosome’s inactivation, which results in a dual expression of TLR7 in the mononuclear cells of women. Functionally, this higher expression of TLR7 is manifested by an increase in the secretion of interferons, a better recognition and elimination of the RNA [ribonucleic acid] virus—as would be the case for the SARS CoV4 virus—and by the stimulation of the production of antibodies against the virus, which in the case of women reach higher and longer-lasting levels than in men (Pisitkun et al, 2006; Berghofer et al, 2006). One interesting fact is that the gene that codifies for the ACE2 molecule is also found in the X chromosome, which promotes a higher presence of this molecule in women (Patel et al, 2014).
The sexual hormones also contribute to the differences in the immune responses of women and of men. The estrogens, the dominant sexual hormone in women, stimulate the innate immune responses and to a lesser degree the adaptive ones, which results in a quicker elimination of pathogens and in the higher efficacy of vaccines in women, as mentioned (Klein & Flanagan, 2016; Jaillon et al, 2017). Inversely, testosterone, the dominant sexual hormone in men, has a suppressive effect on the immune functions, which explains their higher susceptibility to infections (Klein & Flanagan, 2016; Jaillon et al, 2017). To this must be added that the decrease in the levels of testosterone—a characteristic tendency of aging in men—is associated with an increase in the pro inflammatory cytokines (Klein & Flanagan, 2016); Rabi et al, 2020). This fact is one of the features that increase the severity of COVID-19 in older men.
As well as their contribution to the differences in immune responses of women and of men, hormones have an additional mechanism that can influence the pathogenicity of SARS CoV-2 and the severity of COVID-19. This relates to the action of estrogens and testosterone on the ACE2 molecule, the receptor of the virus that penetrates the host cell (Gargaglione & Marques, 2020; Manninga & Fink, 2020).
The ACE2 molecule plays a protective role in some syndromes and chronic diseases, like the before-mentioned comorbidities which affect the course of COVID-19 (Manninga & Fink, 2020). By using ACE2 to enter into the cell in which it will replicate, the virus decreases the availability of the molecule in the affected tissues, particularly in the lungs, and this will make the clinical evolution more complex in cases in which these comorbidities are already present. Estrogen increases the availability of ACE2; testosterone, on the other hand, activates the TMPRSS2 enzyme and, as well as increasing the virus’ penetration, it also decreases the presence of ACE2 (Illustration). Thus, by acting on ACE2 in conflicting manners, estrogen and testosterone can respectively improve or worsen the clinical development of COVID-19 (Gargaglioni & Marques, 2020; Manninga & Fink, 2020).
In all studies, including those dating from before the appearance of COVID-19, the comorbidities previously mentioned (arterial hypertension, cardiovascular diseases, diabetes mellitus and chronic respiratory insufficiency) are more frequent in men than in women (Gebhard et al, 2020). Differences in gender related to unhealthy practices like smoking and drinking alcoholic beverages—which are more frequent in men—have been mentioned as contributing factors (Cai, 2020; Gebhard et al, 2020).
A Chinese publication suggests that, independently of the presence of comorbidities, the custom of smoking is associated with a higher incidence and severity of COVID-19 (Cai, 2020). Another study, also from China, found that this habit was associated with a greater presence of the ACE2 receptor in men, and because of this, with a higher level of the virus’ presence (Zhao et al, 2020). Others have not been able to confirm this cause-and-effect relation and prefer explaining the association based on the chronic inflammation caused by the consumptions of cigarettes, which would predispose the individual to the more severe forms of COVID-19 (Rabi et al, 2020).
Other gender aspects related to the reduced vulnerability of women to COVID-19 are their hygienic habits and healthcare. For example, it has been proven that women are more likely to wash their hands frequently, and to seek medical help when they feel their health is threatened (in COVID-19 cases it has been shown that the earlier the diagnosis is made and treatment begun, the lower are the possibilities of developing the more severe complications of the disease) (Cai, 2020; Gebhard et al, 2020; Zhou et al, 2020b).
By way of epilogue
During the hundreds of years of the practice of medicine, age has been recognized as a factor of great influence in the evolution of diseases; however, the number of professionals who recognize the influence exercised by the variables of sex and gender on the manner of presentation, evolution, diagnostics and treatment of all types of illnesses have only merited space in a small number of academic circles and in a few healthcare sectors.
From a global perspective, the COVID-19 pandemic has unequivocally shown the potential that an appropriate focus on age, sex and gender provides for a more effective practice of medicine. The prevention of the SARS CoV2 infection and, when that has not been possible, its medical treatment and its consequences, has shown the need for a judicious consideration of these variables. We hope that this presentation will help the progress towards a medical practice that, in addition to being universal and gratis—circumstances and determination permitting—, will be precise.
Seen in perspective, the scholarly environment and the pharmaceutical industry cannot turn their backs on these variables. The development of preventive tools, including vaccines, as well as therapeutic procedures, more effective medications among them, all tasks pending since the previous coronavirus pandemics—must take into account the differences presented by age, sex and gender.
Translated by Catharina Vallejo.
Bibliography
Andersen, K., Rambaut, A., Lipkin, W.I., Holmes, E.C., Garry, R.F., 2020. The proximal origin of SARS-CoV-2. Nature Medicine 26, pp.450–452.
Berghofer, B., Frommer, T., Haley, G., Fink, L., Bein, G., Hackstein, H., 2006. TLR7 ligands induce higher IFN-α production in females. Journal of Immunology 177, pp.2088–2096.
Cai, H., 2020. Sex difference and smoking predisposition in patients with COVID-19. Lancet 8, 1. https://doi.org/10.1016/S2213-2600(20)30117-X
Cao, X., 2020. COVID-19: immunopathology and its implications for therapy. Nature Reviews Immunology 20, pp.269–270.
Channappanavar, R., Fett, C., Mack, M., 2017. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. Journal of Immunology 198, pp.4046–4053.
Chen, N., Zhou, M., Dong, X., 2020. Epidemiological and clinica characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet 395, pp.507–513.
Fulop, T., Larbi, A., Dupuis, G., Page, A.L., Frost, E.H., Cohen, A.A., Franceschi, C., 2018. Immunosenescence and inflamm-aging as two sides of the same coin: friends or foes? Frontiers of Immunology 8, p.1960.
Gargaglioni, L.H., Marques, D.A., 2020. Let’s talk about sex in the context of COVID-19. Journal of Applied Physiology 128, pp.1533–1538. https://doi.org/10.1152/japplphysiol.00335.2020
Gebhard, C., Regitz-Zagrosek, V., Neuhauser, H.K., Morgan, R., Klein, S.L., 2020. Impact of sex and gender on COVID-19 outcomes in Europe. Biological Sex Differences 11, pp.1–13. https://doi.org/10.1186/s13293-020-00304-9
Gorbalenya, A.E., Baker, S.C., Baric, R.S., Groot, R.J. de, Drosten, C., Gulyaeva, A.A., Haagmans, B.L., Lauber, C., Leontovich, A.M., Neuman, B.W., 2020. Severe acute respiratory syndrome-related coronavirus: The species and its viruses- a statement of the Coronavirus Study Group. Microbiology.
Goronzy, J.J., Weyand, C.M., 2017. Successful and maladaptive T cell aging. Immunity 46, 364–78.
Hui, D., Madani, T., Ntoumi, F., Kock, R., O, D., 2020. The continuing 2019-nCoV epidemic threat of novel coronaviruses to global health - The latest 2019 novel coronavirus outbreak in Wuhan, China. 2020. International Journal Infection Disease 91, pp.264–266.
Jaillon, S., Berthenet, K., Garlanda, C., 2017. Sexual dimorphism in innate immunity. Clinical Reviews in Allergy & Immunology. https://doi.org/10.1007/s12016-017-8648-x
Klein, S.L., Flanagan, K.L., 2016. Sex differences in immune responses. Nature Reviews Immunology 16, 626–638. https://doi.org/10.1038/nri.2016.90
Kutschera, U., 2020. Gender-specific Coronavirus-infections in the light of evolution. Science 367, pp.1–3.
Lu, R., Zhao, X., Li, J., Niu, P., Yang, B., Wu, H., 2020. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet 395, pp.565–574.
Manninga, J.T., Fink, B., 2020. COVID-19: Digit ratio (2D:4D) and sex differences in national case fatality rates. Early Human Development 146, p.105074. https://doi.org/10.1016/j.earlhumdev.2020.105074
Márquez, E.J., Trowbridge, J.J., Kuchel, G.A., Banchereau, J., Ucar, D., 2020. The lethal sex gap: COVID-19. Immunity & Ageing 17, 1–8. https://doi.org/10.1186/s12979-020-00183-z
Matsuyama, R., Nishiura, H., Kutsuna, S., 2016. Clinical determinants of the severity of Middle East respiratory syndrome (MERS): a systematic review and meta-analysis. BMC Public Health 1203.
MINSAP, 2020. Coronavirus en Cuba. Información oficial del Ministerio de Salud Pública. Junio 28 de 2020.
OMS, 2020. Género. https://www.who.int/health-topics/genero
Patel, S., Velkoska, E., Freeman, M., 2014. From gene to proteinexperimental and clinical studies of ACE2 in blood pressure control and arterial hypertension. Frontiers in Physiology 5 (227).
Pickering, L.A.D., Christie, P., 1980. Sexual differences in the incidence and severity of ectoparasitic infestation of the brown trout, Salmo trutta. Journal Fish Biology 16, pp.669–683. https://doi.org/10.1111/j.1095-8649.1980.tb03746.x
Pisitkun, P., 2006. Autoreactive B cell responses to RNA-related antigens due to TLR7 gene duplication. Science 312, pp.1669–1672.
Qin, C., Zhou, L., Hu, Z., Zhang, S., Yang, S., Tao, Y., Xie, C., Ma, K., Shang, K., Wang, W., 2020. Dysregulation of immune response in patients with COVID-19 in Wuhan, China. Clinical Infectious Diseases. https://doi.org/10.1093/cid/ciaa248
Rabi, F.A., Zoubi, M.S.A., Kasasbeh, G.A., Salameh, D.M., Al-Nasser, A.D., 2020. SARS-CoV-2 and coronavirus disease 2019: what we know so far. Pathogens 9, pp.1–14. https://doi.org/10.3390/pathogens9030231
Schurz, H., Salie, M., Tromp, G., 2019. The X chromosome and sex specific effects in infectious disease susceptibility. Human Genomics 13, pp.1–2.
Shim, E., Mizumoto, K., Choi, W., Chowell, G., 2020. Estimating the risk of COVID-19 death during the course of the outbreak in Korea, February- 1 March, 2020 Case fatality of COVID-19 in Korea 3. Journal of Clinical Medicine 9, 1641. https://doi.org/10.1101/2020.03.30.20048264
Walter, L.A., McGregor, A.J., 2020. Sex- and gender-specific observations and implications for COVID-19. Western Journal of Emergency Medicine 21, p.507. https://doi.org/10.5811/westjem.2020.4.47536
Wang, Y., Wang, Y., Chen, Y., Qin, Q., 2020. Unique epidemiological and clinical features of the emerging 2019 novel coronavirus pneumonia (COVID-19) implicate special control measures. Journal of Medical Virology 92, pp.568–576.
WHO, 2020a. Coronavirus press conference 11 February, 2020.
WHO, 2020b. Virtual press conference on COVID-19 – 11 March 2020.
WHO, 2020c. Coronavirus disease 2019 (COVID-19): Situation report-160. Jun 28. World Health Organization, Geneva.
Yang, J., Zheng, Y., Gou, X., Pu, K., Chen, Z., Guo, Q., Ji, R., Wang, H., Wang, Y., Zhou, Y., 2020. Prevalence of comorbidities in the novel Wuhan coronavirus (COVID-19) infection: a systematic review and meta-analysis. International Journal Infection Disease 94, pp.91–95. https://doi.org/10.1016/j.ijid.2020.03.017
Yurdakök, M., 2020. Sex- and gender-based edicine in pediatrics. Journal of Pediatric and Neonatal Individualized Medicine 9, e090125. https://doi.org/10.7363/090125
Zhao, Y., Zhao, Z., Wang, Y., Zhou, Y., Ma, Y., Zuo, W., 2020. Single-cell RNA expression profiling of ACE2, the putative receptor of Wuhan 2019-nCov. https://doi.org/10.1101/2020.01.26.919985
Zhou, P., L.Yang, X., Wang, X.G., B.Hu, Zhang, L., Zang, W., Si, H.R., Zhu, Y., Li, B., Huang, C.L., 2020a. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 579, pp.270–273.
Zhou, F., Yu, T., Du, R., Fan, G., Liu, Y., and Liu, Z., 2020b. Clinical course and risk factors for mortality of adult inpatients with Covid-19 in Wuhan, China: a retrospective cohort study. Lancet 395, pp.1054–1062.
Deje un comentario